Abstract
Each surgical incision has to be closed after surgery. Suture materials are mostly applied which differ in their filament structure, material composition, as well as in their absorption profile, and the choice of the suture material used for skin closure is mainly based on the surgeon´s preference. We designed a prospective, international, multicentric, single-arm, observational study to assess the clinical outcome of a non-absorbable monofilament nylon-based suture for skin closure with a comparison to historic data from the literature. In total, 115 patients were enrolled with an equally distribution of adults and paediatrics receiving a nylon-based suture material to close the skin. Different safety (wound dehiscence, surgical site infections, and adverse events) and effectiveness parameters (pain, wound healing, patient satisfaction, cosmetic result, intraoperative suture handling) were selected to judge the performance of the suture material. The assessment of patient satisfaction, wound healing, and handling properties of the suture was done using a Likert scale, whereas the Patient and Observer Scar Assessment Scale (POSAS) was chosen for aesthetic scar rating. The primary endpoint was a combined rate of wound dehiscence and surgical site infection occurring until suture removal. After discharge, the patients were examined at suture removal and the paediatric population received a further routinely 1-month post-surgery follow-up. Until suture removal, 2 surgical site infections (1.75%) occurred and one wound dehiscence was seen until 30 days postoperatively, indicating significant lower rates compared to historical data. Furthermore, good handling properties of the suture material as well as a high patient satisfaction combined with an excellent wound healing and cosmetic appearance were reported. Based on our findings, it can be concluded that a monofilament nylon-based suture material is an optimal choice for skin closure in adults as well as in children, and it represents an appropriate alternative to other devices, which are currently in utilization.
Keywords
Suture, Monofilament, Non-absorbable, Skin Closure, Wound Dehiscence, Surgical Site Infection, Cosmetic
1. Introduction
Thousands of surgeries are performed annually worldwide, and nearly all of them involve the approximation of the skin. The wound healing process starts with the wound formation and proceeds in four phases, that occur both sequentially and overlapping: the exudative, resorptive, proliferative, and regenerative phase
.
Various factors such as the type of surgery, method of wound closure, and the patient´s illness, underlying diseases and medication intake influence the wound healing process
.
Besides surgical suture materials, various alternatives such as staples, skin tapes and tissue adhesives are commercially available to approximate the wound edges. Nonetheless, sutures are still mostly used, which differ in their material composition (natural vs. synthetic), filament structure (monofilament vs. multifilament or braided) and degradation profile (non-absorbable vs. absorbable (quick-, mid-term and long-term absorbable). To achieve optimal wound healing, a secure and accurate wound edge adaption is essential. Relevant features of an ideal suture are a combination of good handling properties, minimal tissue reaction, secure knotting, predictable tensile strength and non-allergenic material
. The mechanical properties of different suture materials are probably the most important factors to ensure wound healing with few complications in different anatomic locations and tissues. The choice of the suture material should be based on the biological interaction and the mechanical performance of the material employed, the tissue configuration, and the biomechanical properties of the wound
. The tissue edges need to be held in apposition until the tensile strength of the wound is sufficient to withstand mechanical stress. In this context, the surgeon has to choose not only the suitable suture material, but also the appropriate suture size that the tissue requires which will be approximated. Thus, the choice of suture material in wound management largely depends on factors such as the number of tissue layers involved in wound closure, the tension across the wound, the depth of suture placement, the presence of oedema, the expected time of suture removal, the possession of adequate strength, and the possibility to induce inflammatory reactions. Sutures must also possess significant pliability and flexibility for better handling characteristics during suturing combined with an ease in knot placement and high knot security
| [6] | Dennis C, Sethu S, Nayak S, Mohan L, Morsi YY, Manivasagam G. Suture materials - Current and emerging trends. J Biomed Mater Res A. 2016 Jun; 104(6): 1544-59. https://doi.org/10.1002/jbm.a.35683 |
[6]
.
Non-absorbable sutures have to maintain their tensile strength and are indicated whenever continuous support of the wound is indicated. Several authors considered non-absorbable sutures as the standard method for skin closure
| [7] | Luck RP, Flood R, Eyal D, Saludades J, Hayes C, Gaughan J. Cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations. Pediatr Emerg Care. 2008 Mar; 24(3): 137-42. https://doi.org/10.1097/PEC.0b013e3181666f87 |
| [8] | Luck R, Tredway T, Gerard J, Eyal D, Krug L, Flood R. Comparison of cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations. Pediatr Emerg Care. 2013 Jun; 29(6): 691-5. https://doi.org/10.1097/PEC.0b013e3182948f26 |
| [9] | Theopold C, Potter S, Dempsey M, O'Shaughnessy M. A randomised controlled trial of absorbable versus non-absorbable sutures for skin closure after open carpal tunnel release. J Hand Surg Eur Vol. 2012 May; 37(4): 350-3. https://doi.org/10.1177/1753193411422334 |
[7-9]
. Non-absorbable sutures composed of nylon, polypropylene or polyester are resistant for degradation in vivo and often preferred due to their high tensile strength and minimal inflammatory reaction.
. Additionally, monofilament non-absorbable suture materials are known to have a high memory effect which lead to less knot security and challenging handling
. Furthermore, if these sutures are tied under tension, they can cut the tissue
. In contrast to multifilament sutures, monofilaments pass easily through the tissues because of their smooth surface with a low tissue drag and lack of wicking propensity (capillary effect) which can lead to infections by the penetration of fluids along the suture tract
| [12] | Fowler JR, Perkins TA, Buttaro BA, Truant AL. Bacteria adhere less to barbed monofilament than braided sutures in a contaminated wound model. Clin Orthop Relat Res. 2013 Feb; 471(2): 665-71. https://doi.org/10.1007/s11999-012-2593-z |
| [13] | Lekic N, Dodds SD. Suture Materials, Needles, and Methods of Skin Closure: What Every Hand Surgeon Should Know. J Hand Surg Am. 2022 Feb; 47(2): 160-171.e1. https://doi.org/10.1016/j.jhsa.2021.09.019 |
[12, 13]
. Due to their higher flexibility, multifilament sutures have better handling characteristics in comparison to monofilament sutures.
In total, four meta-analysis/systematic reviews have been carried out so far, comparing the clinical outcome of non-absorbable versus absorbable sutures for skin closure of surgical incisions or traumatic wounds in different locations (face, trunk, limbs, head and neck) in adults and children
| [14] | Malhotra K, Bondje S, Sklavounos A, Mortada H, Khajuria A. Absorbable versus Nonabsorbable Sutures for Facial Skin Closure: A Systematic Review and Meta-analysis of Clinical and Aesthetic Outcomes. Arch Plast Surg. 2024 Jun 19; 51(4): 386-396. https://doi.org/10.1055/a-2318-1287 |
| [15] | Xu B, Xu B, Wang L, Chen C, Yilmaz TU, Zheng W, He B. Absorbable Versus Nonabsorbable Sutures for Skin Closure: A Meta-analysis of Randomized Controlled Trials. Ann Plast Surg. 2016 May; 76(5): 598-606. https://doi.org/10.1097/SAP.0000000000000418 |
| [16] | Al-Abdullah T, Plint AC, Fergusson D. Absorbable versus nonabsorbable sutures in the management of traumatic lacerations and surgical wounds: a meta-analysis. Pediatr Emerg Care. 2007 May; 23(5): 339-44. https://doi.org/10.1097/01.pec.0000270167.70615.5a |
| [17] | Sajid MS, McFall MR, Whitehouse PA, Sains PS. Systematic review of absorbable vs non-absorbable sutures used for the closure of surgical incisions. World J Gastrointest Surg. 2014 Dec 27; 6(12): 241-7. https://doi.org/10.4240/wjgs.v6.i12.241 |
[14-17]
. All reports concluded that non-absorbable suture materials are equivalent to absorbable sutures regarding the rate of surgical site infection, and except for one review, the same result was also mentioned for the wound dehiscence rate
| [17] | Sajid MS, McFall MR, Whitehouse PA, Sains PS. Systematic review of absorbable vs non-absorbable sutures used for the closure of surgical incisions. World J Gastrointest Surg. 2014 Dec 27; 6(12): 241-7. https://doi.org/10.4240/wjgs.v6.i12.241 |
[17]
. Furthermore, the outcome with respect to patient satisfaction, cosmetic appearance and scar formation were also comparable in both suture type groups
| [14] | Malhotra K, Bondje S, Sklavounos A, Mortada H, Khajuria A. Absorbable versus Nonabsorbable Sutures for Facial Skin Closure: A Systematic Review and Meta-analysis of Clinical and Aesthetic Outcomes. Arch Plast Surg. 2024 Jun 19; 51(4): 386-396. https://doi.org/10.1055/a-2318-1287 |
| [15] | Xu B, Xu B, Wang L, Chen C, Yilmaz TU, Zheng W, He B. Absorbable Versus Nonabsorbable Sutures for Skin Closure: A Meta-analysis of Randomized Controlled Trials. Ann Plast Surg. 2016 May; 76(5): 598-606. https://doi.org/10.1097/SAP.0000000000000418 |
[14, 15]
. Non-absorbable sutures analysed in these meta-analyses and systematic reviews were mainly composed of nylon or polypropylene.
The majority of individual randomised controlled trials studies assessing nylon suture materials for surgical skin closure located at the trunk or limbs showed a poor quality according to JADAD scoring and only a few RCTs included a paediatric population
| [15] | Xu B, Xu B, Wang L, Chen C, Yilmaz TU, Zheng W, He B. Absorbable Versus Nonabsorbable Sutures for Skin Closure: A Meta-analysis of Randomized Controlled Trials. Ann Plast Surg. 2016 May; 76(5): 598-606. https://doi.org/10.1097/SAP.0000000000000418 |
| [16] | Al-Abdullah T, Plint AC, Fergusson D. Absorbable versus nonabsorbable sutures in the management of traumatic lacerations and surgical wounds: a meta-analysis. Pediatr Emerg Care. 2007 May; 23(5): 339-44. https://doi.org/10.1097/01.pec.0000270167.70615.5a |
| [17] | Sajid MS, McFall MR, Whitehouse PA, Sains PS. Systematic review of absorbable vs non-absorbable sutures used for the closure of surgical incisions. World J Gastrointest Surg. 2014 Dec 27; 6(12): 241-7. https://doi.org/10.4240/wjgs.v6.i12.241 |
| [18] | Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996 Feb; 17(1): 1-12. https://doi.org/10.1016/0197-2456(95)00134-4 |
[15-18]
. In addition, studies reporting the outcomes with regard to suture handling, patient satisfaction and cosmetic result are also limited
| [16] | Al-Abdullah T, Plint AC, Fergusson D. Absorbable versus nonabsorbable sutures in the management of traumatic lacerations and surgical wounds: a meta-analysis. Pediatr Emerg Care. 2007 May; 23(5): 339-44. https://doi.org/10.1097/01.pec.0000270167.70615.5a |
[16]
.
Therefore, the current study aimed to systematically analyse the clinical outcome of a non-absorbable monofilament nylon-based suture material applied for skin closure of surgical incisions or lacerations localised at the trunk or at the extremities in adults and children under clinical daily practice with a historical comparison to available literature data for nylon suture materials.
2. Materials and Methods
2.1. Registration and Ethical Consideration
In accordance with the Declaration of Helsinki, the present cohort study was proactively registered under www.clinicaltrials.gov on 5 Nov. 2020 [NCT04617041, hyperlink: Study Details | Assessment of DAFILON® Suture Material for Skin Closure | ClinicalTrials.gov], before the first patient was enrolled in the study. Ethics approval was required due to national law. Competent Ethics committees responsible for the participating clinics were contacted and study documents were submitted for approval. The following Institutional Review Boards approved the study design, Ethics Committee, Landesärztekammer Baden-Württemberg (ref. F-2021-035 on 5 March 2021) and Comité de Ética de Investigación con Medicamentos del Hospital Universitario Vall d´Hebron (ref. PR(AMI) 498/2020 on 25 September 2020). Each patient was provided with a written informed consent before inclusion in the study. For the paediatrics population, a written informed consent was obtained from the parents. A study protocol was set up in advance, but not released a priori in a peer-reviewed journal.
The study is reported in alignment with the STROCCS Statement, which is an international standard for publishing observational cohort studies
| [19] | Agha RA, Borrelli MR, Vella-Baldacchino M, Thavayogan R, Orgill DP; STROCSS Group. The STROCSS statement: Strengthening the Reporting of Cohort Studies in Surgery. Int J Surg. 2017 Oct; 46: 198-202. https://doi.org/10.1016/j.ijsu.2017.08.586 |
[19]
.
2.2. Design, Participants and Settings
A prospective, international, bicentric, single-arm cohort study was chosen as a design to systematically investigate the clinical performance of a monofilament nylon- based suture material applied for skin closure in adults and children under clinical routine conditions. Two high- volume clinics located in Spain (paediatric surgery) and in Germany (visceral surgery) were selected for participation because these clinics have used the nylon-based suture material for skin approximation for years and they were familiar with the application of the device and therefore, representative data were generated with high transferability and generalisation potential. Both clinics consecutively recruited their patients from the population treated at the hospital as part of daily practice according to the local standard.
Screened and eligible patients were operated and followed-up until day of discharge and day of suture removal (approx. 10 days ±5 d postop), whereby an additional routine follow-up examination was performed in the paediatric population 1 month after surgery (
Figure 1). Enrolment took place between March 2021 and March 2022. Postoperative follow-up examination was completed in June 2023. The first patient was recruited on 11 March 2021, the last patient was enrolled on 25 May 2023 and completion of the one-month post-surgery visitation was performed on 15 June 2023. The study was regularly finished.
Paediatric and adult patients undergoing routine skin closure of linear, minimally contaminated incisions or lacerations located at the trunk or limbs, which provided their written informed consent, were eligible for participation. Emergency surgery, fascial lacerations or incisions, contaminated wounds, nonlinear shape, hypersensitivity or allergy against nylon and use of medication that might affect wound healing (e.g. immunosuppressive medication) were selected as exclusion criteria. The nylon-based suture material, named Dafilon® and manufactured by B. Braun Surgical SA, Rubi, Barcelona, Spain, was used for skin closure. Dafilon® is a sterile, monofilament non-absorbable suture produced from polyamide. It is available undyed or coloured in blue or black. USP sizes range from 5 to 6/0 and are intended to be used for soft tissue approximation in the skin. The USP size of the suture material and the suture technique (continuous intradermal or interrupted transcutaneous) applied for skin approximation were chosen by the surgeon.
Data collected for the current study were recorded on paper-based Case Report Forms (CRF) which were verified regarding their correctness, plausibility and completeness by trained monitors during regular visits performed in both hospitals. The CRFs were transferred by the monitors to the data management centre for data entry in a validated electronic data capture system owned by the study sponsor. To ensure quality and reliability of the dataset, a double data entry was performed by data management. Inconsistency of the data was clarified with the hospitals using data clarification sheets (DCRs) handed over by the monitor to the investigator for clarification. The department of the sponsor responsible for project management, monitoring, data management and biometry was externally audited in March 2021.
2.3. Outcomes
2.3.1. Primary Objective
The primary outcome of the study was a combined endpoint including the rate of surgical site infection (SSI) and wound dehiscence until day of suture removal (approximately 10 days ±5 d after surgery). SSI were classified according to the Centers for Disease Control and Prevention (CDC), and SSI of type A1 (superficial) and A2 (deep) were reported and included in the primary endpoint. A wound dehiscence was defined as a partial or complete diverge of the wound margins adapted by the suture material; the dehisced wound may, or may not, display signs and symptoms of infection.
2.3.2. Secondary Parameter
The safety assessment of the suture material was performed by analysing the incidence of SSI, wound dehiscence, tissue reaction, allergy reaction, seroma or abscess formation, haematoma, as well as the need for premature suture removal or re-suturing until the day of suture removal or 1-month post-surgery in the paediatric population.
Each safety parameter was assessed for intensity (mild, moderate, severe) and seriousness. Events that fulfilled one of the following categories were rated as serious: required or prolonged hospitalisation, need for medical treatment or surgery to prevent impairment of a body structure or function, life threatening event or death. In addition, serious adverse events were recorded with respect to causal relationship to the medical device and expectedness.
Effectiveness was evaluated based on the outcome of the scar quality, wound healing assessment, pain level, pain duration, and patient´s satisfaction. The aesthetic result of the scar was rated using an international, validated and reliable measure named POSAS (Patient and Observer Scar Assessment Scale)
| [20] | Draaijers LJ, Tempelman FR, Botman YA, Tuinebreijer WE, Middelkoop E, Kreis RW, van Zuijlen PP. The patient and observer scar assessment scale: a reliable and feasible tool for scar evaluation. Plast Reconstr Surg. 2004 Jun; 113(7): 1960-5; discussion 1966-7. https://doi.org/10.1097/01.prs.0000122207.28773.56 |
| [21] | van de Kar AL, Corion LU, Smeulders MJ, Draaijers LJ, van der Horst CM, van Zuijlen PP. Reliable and feasible evaluation of linear scars by the Patient and Observer Scar Assessment Scale. Plast Reconstr Surg. 2005 Aug; 116(2): 514-22. https://doi.org/10.1097/01.prs.0000172982.43599.d6 |
| [22] | Truong PT, Lee JC, Soer B, Gaul CA, Olivotto IA. Reliability and validity testing of the Patient and Observer Scar Assessment Scale in evaluating linear scars after breast cancer surgery. Plast Reconstr Surg. 2007 Feb; 119(2): 487-94. https://doi.org/10.1097/01.prs.0000252949.77525.bc |
[20-22]
. It is a comprehensive scale designed for evaluating all types of scars by professionals and patients [https://www.posas.org]. The medical staff used the Observer component of the POSAS to assess the cosmetic outcome of the wound. The Observer component of the POSAS scale evaluates 6 different dimensions and each dimension has a 10-level rating scale from 1 [normal skin] to 10 [worst scar imaginable]. The Observer component of the POSAS consists of the following criteria: 1) vascularity (presence of vessels in the scar tissue assessed by the amount of redness tested by the amount of blood return after blanching with a piece of Plexiglas; 2) pigmentation (brownish coloration of the scar by pigmentation; apply transparent plexiglass to the skin with moderate pressure to eliminate the effect of vascularity; 3) thickness (average distance between the subcuticular-dermal border and the epidermal surface of the scar; 4) relief (the extent to which surface irregularities are present, preferably compared with adjacent normal skin); 5) pliability (suppleness of the scar tested by wrinkling the scar between the thumb and index finger); 6) surface area (surface area of the scar in relation to the original wound area). The patient component of POSAS includes six questions which had to be answered on a 10-point Likert scale (1 like normal to 10 very different from normal skin). In the present study, the assessment in the paediatric subgroup was mainly made by the parents because most of the children were too young to evaluate on their own. The POSAS score ranges from 6 points minimum to 60 points maximum for each component.
Wound healing was judged by the physician using a Likert scale ranging from 0 (very poor) to 100 (excellent) points. Additionally, the physician reported if a hypertrophic or keloid scar was present. The duration and level of pain were assessed by the patient, whereby the Visual Analogue Scale (VAS), a frequently used method for pain intensity, consisting of a horizontal 10 cm scale labelled at each end by descriptors such as “0 = no pain and 100 = highest pain ever”, was used for pain grading. Furthermore, patients appraised their satisfaction using a numerical 100- point scale with a range of 0 = unsatisfied to 100 = extremely satisfied.
Intraoperatively, the handling characteristics of the suture material during the skin approximation were rated by the surgeons and a questionnaire was completed after each surgery. As handling categories, knot security, knot run down, tensile strength, tissue drag and pliability were selected, and performance was reported on a 5- point Likert scale as follows: 1 (excellent), 2 (very good), 3 (good), 4 (satisfied) and 5 (poor).
2.4. Sample Size and Statistical Methods
2.4.1. Statistical Hypothesis
To compare the primary outcome of a monofilament non-absorbable nylon-based suture material, the Systematic Review (SR) published by Sajid et al., which analysed non-absorbable versus absorbable suture materials for skin closure of surgical incisions, served as a historical control
| [17] | Sajid MS, McFall MR, Whitehouse PA, Sains PS. Systematic review of absorbable vs non-absorbable sutures used for the closure of surgical incisions. World J Gastrointest Surg. 2014 Dec 27; 6(12): 241-7. https://doi.org/10.4240/wjgs.v6.i12.241 |
[17]
.
The focus of comparison of the current study was on a composite endpoint that incorporates the main complications occurring after skin closure, namely surgical site infection and wound dehiscence. Therefore, the findings of 6 RCTs using suture materials composed of nylon included in the SR of Sajid et al. were summarised regarding the rates of surgical site infection and wound dehiscence, and were used for comparison. The sum of wound dehiscence and surgical site infection rate was 13% for non-absorbable nylon-based suture materials
| [23] | Foster GE, Hardy EG, Hardcastle JD. Subcuticular suturing after appendicectomy. Lancet. 1977 May 28; 1(8022): 1128-9. https://doi.org/10.1016/s0140-6736(77)92385-6 |
| [24] | Kotaluoto S, Pauniaho SL, Helminen M, Kuokkanen H, Rantanen T. Wound healing after open appendectomies in adult patients: a prospective, randomised trial comparing two methods of wound closure. World J Surg. 2012 Oct; 36(10): 2305-10. https://doi.org/10.1007/s00268-012-1664-3 |
| [25] | Lundblad R, Simensen HV, Wiig JN, Niels Grüner OP. Hudlukning. [Skin closure. A prospective randomized study]. Tidsskr Nor Laegeforen. 1989 Apr 30; 109(12): 1307-9. |
| [26] | Pauniaho SL, Lahdes-Vasama T, Helminen MT, Iber T, Mäkelä E, Pajulo O. Non-absorbable interrupted versus absorbable continuous skin closure in pediatric appendectomies. Scand J Surg. 2010; 99(3): 142-6. https://doi.org/10.1177/145749691009900308 |
| [27] | Ralphs DN, Cannon SR, Bolton JP. Skin closure of inguinal herniorrhaphy wounds in short-stay patients. Br J Surg. 1982 Jun; 69(6): 341-2. https://doi.org/10.1002/bjs.1800690617 |
| [28] | Szabó S, István G. Inguinális sérvmútétek bórvarrata gyorsan felszívódó Polyglactin 910/370 (Vicryl-Rapide) fonallal [Skin closure in inguinal hernia repair with rapidly absorbing Polyglactin 910/370 (Vicryl-Rapide) suture material]. Magy Seb. 2002 Apr; 55(2): 77-80. |
[23-28]
. The decision for taking the findings of these 6 RCTs from the SR for comparison was first the availability of clinical data for non-absorbable nylon-based suture materials, second the generation of clinical data in European countries and third the skin closure of surgical incisions located at the trunk. All these factors were relevant for the comparability of our results.
The hypothesis of the current study was that the combined endpoint consisting of the surgical site infection and wound dehiscence rate is not inferior to the rate of 13%. To set up an inferiority margin, the highest complication rate of surgical site infection and wound dehiscence published in the 6 individual RCTs were combined and led to 25.3%. For our study we chose an inferiority margin of maximal 7%. Therefore, with a non-inferiority margin of 7.0%, rates of M = 20.0% or more were considered as inacceptable.
2.4.2. Sample Size
The study proved the hypothesis of non-inferiority of p(test) = 13.0% to the margin M = 20.0%. For a two-sided 95% Agresti-Coull confidence interval for binominal proportion whose true value is 0.13, a sample size of n= 108 yields a half-width of at most 0.07 with a conditional probability of 0.80. This sample size is based on an expected cumulative complication rate of 13.0% and an inferiority margin lying 7% over the expected rate. Including a drop-out rate of 5%, the number of patients to be recruited increases up to n=114 patients (108/(100-5)*100). Therefore, a total of 114 patients were enrolled in the current study with an equal distribution of adult and paediatric patients (n = 57 patients each).
2.4.3. Statistical Analysis
All patients receiving the non-absorbable monofilament nylon-based suture material for skin closure were included in the per-protocol analysis. For statistical analysis, SAS V04.00 (SAS Institute Inc.; Cary, NC, USA) was used. Missing values were analysed as such and no replacement was done. For summary results (mean, standard deviation), the number of data were listed. To identify the data of the patient, the study centre ID and patient ID assigned during data entry were used.
The following guidelines were applied for statistical analysis: Variables with metric or ordinal scale were summarised as follows: N observations, Min, Max, Median, Mean, Standard Deviation (StD). Optional: missing data (Nmiss), upper and lower quartiles (Q3 and Q1), 95% confidence interval of the median, and pre-specified test p values. Categorical variables were summarised by categories: Number of observations (N), Relative frequencies (p, %). A "N/A" category identified missing values. The following standard comparison methodologies were employed: Chi-Square test for binary data, U-test using Wilcoxon-Mann-Whitney or Kruskal-Wallis for non-parametric data, t test or One-Way-ANOVA for metric data assuming a normal distribution. Statistics (box plots, bar charts) were used when applicable. The sponsor was responsible for the organisation of the study data statistical analysis. Statistical tests were two-tailed or one-tailed with alpha = 5% or 2.5%, respectively. Thus, two-sided 95% confidence intervals were used. The primary variable test was confirmatory, all other tests explanatory. The explanatory test p-values may indicate a difference in the sample rather than the population. For the identification of relevant influencing factors and parameters of primary and secondary variables, multivariate regression models were used when appropriate. Depending on the outcome parameter, linear or logistics models were implemented. In these models, the patient age, gender, BMI and respective baseline value were used as covariates.
3. Results
3.1. Recruitment, Population and Visitations
A total of 121 patients were screened and checked for eligibility. Finally, 115 subjects were enrolled and their skin was closed using the monofilament, non-absorbable nylon- based suture material. Six patients were not included because they violated the inclusion criteria “nylon-based suture material applied to approximate the skin” and therefore, these patients were intraoperatively excluded. The study population comprised of 57 adults enrolled in the German clinic and 57 paediatrics and one adult recruited in the Spanish clinic. During the monitoring visitation, it was realized that one Spanish patient was older than 18 years and therefore, it was decided that this patient should stay in the study, but for analysis purposes this patient was moved to the adult group. The analysed SKINDA cohort consisted of 58 adult and 57 paediatric patients (
Figure 1).
Figure 1. Flow chart of the study.
The dataset of 115 patients was available until the day of discharge and one adult patient was lost to follow-up for the visitation “day of suture removal”. All Spanish patients received the 1-month post-surgery visit (57 children and 1 adult), whereas adults enrolled in Germany completed the study after suture removal (approx. after 10 days postoperatively.).
3.2. Demography and Baseline Characteristics
Demographic data such as gender, age, weight, height and BMI are shown in
Table 1. The cohort encompassed thirty-five females (30%) and 80 males (70%). Gender distribution was equal in the paediatric population with 26 girls and 31 boys, whereas the adult group included mainly males (N= 49/58, 84%), depending on the reason for surgery (inguinal hernia repair) in the adult group, which will be further described in the section “intraoperative data”.
The adult group averaged 62.09 ±16.01 years of age and the median BMI of adults was 25.06 (17.92 – 40.17) kg/m2. The paediatric group included 2 infants (≤1 year), 44 children (> 1- 11 years) and 11 adolescent patients (> 11-18 years). The mean age of the paediatric group was 6.57 ±4.13 years [range 0.3 years - 16 years]. Obese patients were seen in both subgroups with 9% in each group (adults and paediatrics) having a BMI greater than 30 kg/m2.
Risk factors known to influence the wound healing outcome were collected preoperatively and reported only in the adult population, which included 23% current smokers, and 12% diabetic patients; of these, one patient was insulin-dependent (data not shown).
3.3. Intraoperative Details
3.3.1. Reason for Surgery and Localisation of the Incision
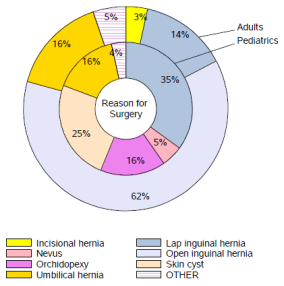
The reason for surgery was mainly inguinal hernia repair in the whole study cohort (N= 64/115, 56%),
Figure 2. The majority of adults received an open inguinal hernia surgery (N= 36/58, 62%), whereas in paediatrics this surgical intervention was performed laparoscopically (N= 20/57, 35%). Skin cyst removal (N= 14/57, 25%), umbilical hernia repair (9/57, 16%) and orchidopexy 9/57, 16%) were reported as further indications for surgery in the paediatric group. The removal of a nevus, an incisional or epigastric hernia repair or the performance of a cholecystectomy were rarely reported and below 3%.
The mean duration of surgery in adults was more than twice as long compared to paediatrics,
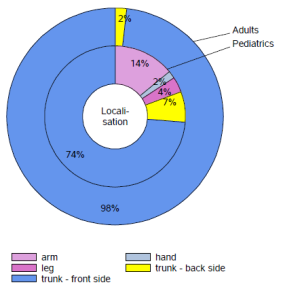
Table 2. Surgical incisions were predominately localised in both subgroups on the front side of the trunk (86%), as illustrated in
Figure 3.
Figure 2. Reason for surgery depending on subgroups.
Figure 3. Location of the incision depending on subgroups.
Table 1. Demographic data of the study cohort and depending on subgroups.
Parameter | Subgroups | Number (N) | Median (Range) | Mean (SD) |
Gender | All | 115 | | |
Females | 35 |
Males | 80 |
Gender Adults | Adults | 58 |
Females | 26 |
Males | 32 |
Gender Paediatrics | Paediatrics | 57 |
Females | 9 |
Males | 48 |
Age (years) | All | 115 | 18.0 (0.30 – 88.0) | 34.6 (30.2) |
Adults | 58 | 62.5 (18.0 – 88.0) | 62.1 (16.1) |
Paediatrics | 57 | 6.0 (0.30 – 16.0) | 6.6 (4.1) |
Weight (kg) | All | 115 | 60.0 (7.0 – 145.0) | 54.3 (30.5) |
Adults | 58 | 81.5 (46.0 – 145.0) | 80.6 (13.9) |
Paediatrics | 57 | 22.0 (7.0 – 80.0) | 27.5 (15.8) |
Height (cm) | All | 115 | 160.0 (60.0 – 192.0) | 145.6 (38.8) |
Adults | 58 | 178.0 (153.0 – 192.0) | 176.9 (9.1) |
Paediatrics | 57 | 105.0 (60.0 – 175.0) | 113.8 (30.5) |
Body Mass Index (BMI) (kg/m2) | All | 115 | 23.1 (12.7 – 40.2) | 23.1 (5.1) |
Adults | 58 | 25.1 (17.9 – 40.2) | 25.7 (3.7) |
Paediatrics | 57 | 19.4 (12.7 – 33.4) | 20.4 (5.0) |
In 15 paediatric patients, the skin was incised at another body region such as at the arm, leg, hand and on the back side of the trunk. The length of the surgical incision was markedly longer in the adult group compared to the paediatric group,
Table 2. In paediatrics, the skin was mainly closed using the intracutaneous-continuous suture technique (93%), as opposed to adults, whose skin was approximated applying the transcutaneous-interrupted suture technique (97%). The Spanish paediatric surgeons preferred USP size 5/0 combined with a DS 16 mm needle, whereas the German general surgeons (adult subgroup) mostly used USP size 3/0 attached to a DS 24 mm needle.
3.3.2. Intraoperative Handling of the Suture Material
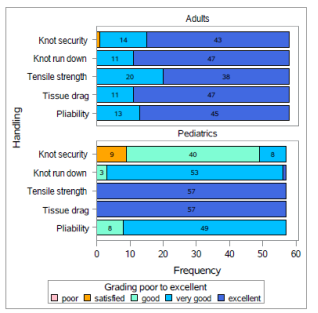
All handling dimensions were rated by the surgeons of the adult group predominately with 1-2 points, indicating that the handling of the nylon suture material was very good to excellent (
Figure 4). The paediatric surgeons judged the categories tensile strength and tissue drag as excellent in 100% of the cases, the dimensional pliability, knot run down and knot security received a good to very good assessment, whereby in 9 paediatric surgeries the parameter “knot security” obtained a satisfactory rating.
Figure 4. Frequency shown in bar diagrams of the assessed handling parameter of the suture material.
3.4. Length of Hospital Stay and Time to Suture Removal
Most of the adult patients stayed in the hospital for 2 days. Children left the clinic on the same day of surgery or one day post-surgery, see
Table 2.
The suture material was removed in the whole population after an average duration of 10 days after the initial surgery, whereby the suture removal was done 5 days earlier in the paediatric group compared to the adult group (
Table 2).
3.5. Complications and Adverse Events
3.5.1. Primary Endpoint of the Study
The primary endpoint of the study was the combined rate of surgical site infection and wound dehiscence until suture removal. We detected only 2 SSIs of class A1 (superficial) and no wound dehiscence until the day of suture removal, which leads to a complication rate of 1.75% (N =2/114) in the SKINDA study compared to 13% in the historical control group. Our findings indicate that using a monofilament non-absorbable nylon-based suture material (Dafilon®) for skin closure a significant lower complication rate can be obtained compared to the literature data (1.75% CI 95% [0.09% -6.57%], p <0.001).
Since both SSIs were seen in the paediatric group, we performed also a subgroup analysis regarding the primary endpoint, which showed the following results:
Adults: N= 0/57; 0.00%; CI 95% [0.00% - 7.55%]; p > 0.0001
Children: N= 2/57; 3.51%; CI 95% [0.27% - 12.61%], p= 0.001
One SSI occurred in a 12-year-old boy after an inguinal hernia repair and the 2nd SSI was observed in a 9-year-old girl after umbilical hernia repair. Both incisions (1-2 cm) were closed using the intracutaneous-continuous suture technique. Both events were recorded as mild, non-serious, unexpected and with no causal relationship to the suture material. In none of the cases the suture material was removed prematurely. The events were treated with antibiotics and resolved with no sequalae. A possible contamination during surgery was given as a reason for SSI development.
3.5.2. Other Adverse Events
Intraoperatively, neither an adverse event nor a device deficiency occurred. One subcutaneous haematoma was diagnosed in an adult male patient (71 years old, open inguinal hernia repair, transcutaneous-interrupted suture, incision length 18 cm) until day of discharge, which required a revision and led to a haematoma rate of 1.75% in the adult group (N=1/57) and 0.87% for the total population (N= 1/115;), respectively. The event was classified as moderate and serious, because hospitalisation was extended due this event. The event resolved with no sequelae and neither a causal relationship with the suture material nor with the surgical procedures was reported. Furthermore, the event was documented as expected, because the patient was under anti-coagulopathy treatment. A mild, non-serious seroma was mentioned in a 3-year-old child after umbilical hernia repair, which was drained and resolved with no sequalae. A wide dissection was given as a possible reason for development. A further complication was recorded in the paediatric group until 30 days after surgery. A mild, non-serious, unexpected wound dehiscence occurred in a 4-year-old girl after the removal of a skin cyst, whereby the 1 cm incision was approximated using a transcutaneous-interrupted suture. Care treatment was applied and the event resolved with no sequalae and no causal relationship neither to suture material nor to the surgical procedure was mentioned. In sum, 5 adverse events occurred in the whole study population until 30 days after surgery, 4 events in the paediatric group (2 SSIs, 1 seroma, 1 wound dehiscence) and one in the adult group (one haematoma). A subgroup analysis of the SSI and wound dehiscence rate in the paediatric group 30 days after surgery showed the following numbers:
Surgical site infection and wound dehiscence until 30 days after surgery in children: N= 3/57; 5.26%%; CI 95% [1.24% - 14.94%].
Wound dehiscence until 30 days after surgery in children: N= 1/57; 1.75%; CI 95% [0.00% - 10.17%]
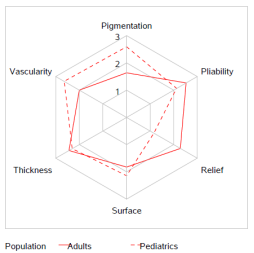
3.6. Postoperative scar assessment using POSAS
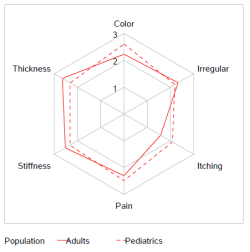
On the day of suture removal, the scar quality was assessed by professional medical staff and patients/parents using the POSAS questionnaire. The outcome regarding the overall opinion of the patient was similar to the overall opinion of the physician (2.26 vs. 2.05) and indicated an excellent cosmetic result independent of the assessor. We performed also a subgroup analysis of the different POSAS dimensions with respect to adults and paediatrics, because the skin maturity differs between these groups. The categories pain, thickness, stiffness and irregularity showed comparable values in both patient groups (
Figure 5). In contrast, the parameters “itching and colour” showed higher values in the paediatric group on the day of suture removal, indicating that the wound area differed more from normal skin compared to the wounds of the adults. In accordance with these findings, a significant higher value was given by the observers for the categories “pigmentation and vascularity” in the children group, whereas the dimensions “relief and pliability” was rated significantly poorer by the observers in the adult group (
Figure 6).
Figure 5. Patient assessment of scar quality at suture removal.
Figure 6. Observer assessment of scar quality at suture removal.
Table 2. Intraoperative and postoperative outcome parameter.
Parameter | Group | N | Median (range) | Mean (SD) |
Hospital stay (days) | All | 115 | 0.0 (0.0 – 12.0) | 0.98 (1.69) |
Adults | 58 | 0.0 (0.0 – 12.0) | 1.91 (1.98) |
Paediatrics | 57 | 0.0 (0.0 – 1.0) | 0.04 (0.19) |
Time to suture removal (days) | All | 114 | 9.0 (5.0– 17.0) | 9.65 (2.95) |
Adults | 57 | 13.0 (7.0 – 17.0) | 11.91 (2.21) |
Paediatrics | 57 | 7.0 (5.0 – 14.0) | 7.39 (1.52) |
Length of incision (cm) | All | | | |
Adults | 58 | 6.0 (1.00– 18.0) | 6.14 82.89) |
Paediatrics | 57 | 2.0 (1.0 – 3.0) | 1.63 (0.70) |
Duration of operation (minutes) | All | | | |
Adults | 58 | 54.5 (12.0 –127.0) | 58.86 (20.81) |
Paediatrics | 57 | 20.0 (10.0 – 50.0) | 22.28 (8.65) |
Duration of pain after surgery (days) At suture removal Number of patients with pain At suture removal | All | 100 | 3.0 (1.0 – 14.0) | 4.35 (2.61) |
Adults | 45 | 6.0 (2.0 – 14.0) | 5.87 (3.06) |
Paediatrics | 55 | 3.0 (1.0 – 7.0) | 3.11 (1.17) |
All | 114 | | |
Adults | 8/57 | | |
30 days postop | Paediatrics | 2/57 | | |
Paediatrics | 0/57 | | |
Pain intensity (VAS) At discharge At suture removal 30 days postop | All | 115 | 20.0 (0.0 – 100.0) | 25.77 (17.28) |
Adults | 58 | 20.0 (0.0 – 100.0) | 23.34 (19.96) |
Paediatrics | 57 | 30.0 (10.0 – 80.0) | 28.25 (13.77) |
All | 114 | 20.0 (0.0 – 100.0) | 22.54 (21.07) |
Adults | 57 | 10.0 (0.0 – 100.0) | 24.21 (28.41) |
Paediatrics | 57 | 20.0 (10.0 – 60.0) | 20.88 (9.12) |
Paediatrics | 57 | 20.0 (10.0 – 60.0) | 20.70 (9.23) |
Patient satisfaction (VAS) At discharge At suture removal 30 days postop | All | 115 | 100.0 (0.0 –100.0) | 92.48 (13.12) |
Adults | 58 | 90.0 (0.0 – 100.0) | 90.60 (14.87) |
Paediatrics | 57 | 100.0 (30.0–100.0) | 94.39 (10.86) |
All | 114 | 100.0 (0.0 –100.0) | 93.71 (14.06) |
Adults | 57 | 100.0 (0.0– 100.0) | 90.58 (18.08) |
Paediatrics | 57 | 100.0 (60.0–100.0) | 96.84 (7.36) |
Paediatrics | 57 | 100.0 (80.0–100.0) | 97.37 (5.83) |
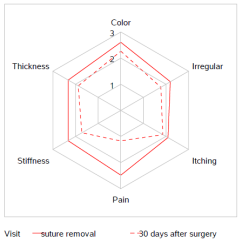
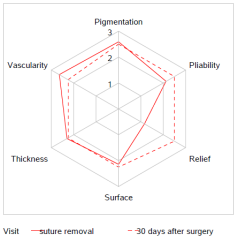
The routine follow-up examination in children performed 30 days after surgery showed an improvement of all patient component dimensions from day of suture removal until 1-month post-surgery indicated an excellent scar appearance. Furthermore, the patient´s and observer´s aesthetic assessment was largely consistent (
Figures 7, 8).
3.7. Postoperative Pain Assessment, Patient Satisfaction and Wound Healing Result Using the VAS
The outcome with regard to pain, wound healing assessment and patient satisfaction is shown in
Tables 2, 3. If the child was too young to evaluate the parameter on his/her own, the judgement was performed by the parents. The majority of individuals (87%) had pain after surgery until the day of discharge. Pain level was slightly higher in paediatrics in comparison to adults. A decrease in the number of patients suffering from pain as well as the pain level was noted on the day of suture removal. In total, 87% of the patients were pain free on the day of suture removal. Pain was present in the whole cohort for approximately 4 days after surgery, whereby the maximal pain duration was 7 days longer in the adult group (min. 2d – 14 d max.) compared to the paediatric group (min. 1d – max. 7d). Pain medication was necessary on the day of discharge in all paediatrics and in 71% of the adults. Intake of painkillers was only needed in one child and in 7 adults on the day when the suture was removed. No pain and no need to take pain medication was reported in the paediatric group 30 days post-surgery.
The scar was assessed by the physicians on the day of suture removal and additionally in children 30 days after surgery. Neither a hypertrophic scar nor keloids were reported in the whole study population. The average physician´s wound healing evaluation was excellent at suture removal (98.23 ± 3.81), with no difference in the subgroups.
Figure 7. Paediatrics assessment of scar quality at suture removal and 30 days postoperatively.
Figure 8. Observer assessment of scar quality at suture removal and 30 days postoperatively.
Patients assessed their satisfaction on the day of suture removal and in the paediatric group a further assessment was done 1 month after surgery. Patient satisfaction was high at different time points and a comparison between adults and children showed a better rating in the paediatric group.
Table 3. POSAS outcome depending on subgroups and visitations.
Parameter | Group | N | Median (range) | Mean (SD) |
POSAS: Overall opinion patient At suture removal 30 days postop | All | 113 | 2.00 (1.00-4.00) | 2.36 (0.72) |
Adults | 57 | 2.00 (1.00-4.00) | 2.40 (0.86) |
Paediatrics | 56 | 2.00 (1.00-4.00) | 2.32 (0.54) |
Paediatrics | 57 | 2.00 (1.00-3.00) | 1.88 (0.54) |
POSAS: Overall opinion observer At suture removal 30 days postop | All | 113 | 2.00 (1.00-4.00) | 2.05 (0.58) |
Adults | 57 | 2.00 (1.00-4.00) | 1.98 (0.74) |
Paediatrics | 56 | 2.00 (1.00-3.00) | 2.13 (0.33) |
Paediatrics | 4 | 2.50 (2.00-4.00) | 2.75 (0.96) |
POSAS: Patient score At suture removal 30 days postop | All | 113 | 14.00 (7.00-23.00) | 13.81 (3.28) |
Adults | 57 | 13.00 (7.00-23.00) | 13.61 (3.82) |
Paediatrics | 56 | 14.00 (9.00-22.00) | 14.02 (2.65) |
Paediatrics | 57 | 10.00 (7.00-18.00) | 10.67 (2.47) |
POSAS: Observer score At suture removal 30 days postop | All | 113 | 13.00 (6.00-23.00) | 12.83 (3.16) |
Adults | 57 | 12.00 (6.00-12.00) | 12.70 (4.14) |
Paediatrics | 56 | 13.00 (9.00-17.00) | 12.96 (1.69) |
Paediatrics | 4 | 13.00 (9.00-22.00) | 4.25 (5.74) |
Wound healing assessment by the physician (VAS) At discharge | All | 115 | 100.0 (90.0-100.0) | 98.78 (3.22) |
Adults | 58 | 100.0 (90.0-100.0) | 98.10 (3.84) |
Paediatrics | 57 | 100.0 (90.0-100.0) | 99.47 (2.25) |
At suture removal 30 days postop | All | 114 | 100.0 (80.0-100.0) | 98.23 (3.81) |
Adults | 57 | 100.0 (80.0-100.0) | 96.81 (4.67) |
Paediatrics | 57 | 100.0 (90.0-100.0) | 99.85 (1.86) |
Paediatrics | 4 | 100.00 (80.00-100.0) | 95.00 (10.00) |
4. Discussion
The final aesthetic outcome of the scar is influenced by multiple factors, such as skin type, localization on the body, suture material and technique, wound management and the tension of the wound margins. The course of wound healing and the final appearance of the scar are impacted by surgical strategies and surgical practice
. To achieve optimal wound healing, wound edges should be aligned in a proper way, whereby wound cavities, layered wound closure and everted wound edges should be avoided. To minimize the risk for infection, necrosis, excessive scarring and wound dehiscence, tension on the wound should be omitted
. Furthermore, the appearance of the surgical scars has a great influence on the patient´s physical and psychological well-being, and the choice of skin closure method has an impact on both patient outcome and healthcare resources.
There are many different suture materials and suture techniques available for primary wound closure. Selection depends on the defect size, anatomic location, presence and absence of tension, and the preference and skill level of the surgeon.
A similar risk for wound infection and other postoperative complications was shown when non-absorbable suture materials were compared to absorbable sutures
| [17] | Sajid MS, McFall MR, Whitehouse PA, Sains PS. Systematic review of absorbable vs non-absorbable sutures used for the closure of surgical incisions. World J Gastrointest Surg. 2014 Dec 27; 6(12): 241-7. https://doi.org/10.4240/wjgs.v6.i12.241 |
[17]
. Furthermore, no difference in scar quality was mentioned between absorbable and non-absorbable sutures
| [31] | Vogt PM, Altintas MA, Radtke C, Meyer-Marcotty M. Grundlagen und Techniken der chirurgischen Naht [Bases and methods of suturing]. Chirurg. 2009 May; 80(5): 437-44, 446-7. German. https://doi.org/10.1007/s00104-009-1670-7 |
[31]
. Suture materials consisting of a monofilament fibre- induced fewer tissue reactions than multifilament or braided suture materials.
The present study assessed the safety and effectiveness of a non-absorbable monofilament suture material for skin closure after open or laparoscopic interventions in adults and paediatrics treated in daily clinical routine in two European countries, whereby the suture technique was selected based on the surgeon´s preference. The incidence and severity of postoperative complications are key elements in determining the risk/benefit ratio of any surgical procedures. Short term complications after skin closure include wound infection and wound dehiscence. Therefore, we choose a combination of surgical site infection and wound dehiscence rate until suture removal as the primary outcome of the current study.
Until suture removal, we observed only 2 surgical site infections (2/114; 1.75%) and one wound dehiscence developed between suture removal and 30 days after surgery (1/57, 1.75%) in a 4-year-old girl after removal of a skin cyst in the hand region. A transcutaneous, interrupted suture technique was chosen to close the 1 cm high-tension excisional wound, whereas for the other paediatric surgical wounds, an intracutaneous-continuous suture technique was mostly selected (93%). Therefore, the chosen suture technique could be a reason for the observed wound dehiscence, because Luo et al. recommended in their meta-analysis that when dealing with skin closure in high tension areas, an intracutaneous continuous suture is a better method to reduce the complication of wound opening
| [32] | Luo W, Tao Y, Wang Y, Ouyang Z, Huang J, Long X. Comparing running vs interrupted sutures for skin closure: A systematic review and meta-analysis. Int Wound J. 2023 Jan; 20(1): 210-220. https://doi.org/10.1111/iwj.13863 |
[32]
. Furthermore, Luo and colleagues were able to show that a continuous suture (intradermal or subcutaneous) is superior to the interrupted suture for skin closure of non-obstetric or traumatic wounds in terms of wound healing and cosmetic appearance. In their meta-analysis, mainly nylon-based sutures were applied for skin closure when a non-absorbable suture material was selected
| [32] | Luo W, Tao Y, Wang Y, Ouyang Z, Huang J, Long X. Comparing running vs interrupted sutures for skin closure: A systematic review and meta-analysis. Int Wound J. 2023 Jan; 20(1): 210-220. https://doi.org/10.1111/iwj.13863 |
[32]
.
A wound dehiscence is an infrequent and rare complication in children, occurring in less than 1% of surgical patients following intra-abdominal surgery according to Waldhausen and Singer
. Furthermore, Campbell and Swenson reported an incidence of 0.2% - 3.3/% in paediatrics after abdominal surgery, depending on the type of incision
. Waldhausen et al. analysed the influence of the type of incision (transverse versus vertical) on wound dehiscence in children undergoing intraabdominal surgery
. Vertical incisions were found to be much more likely to dehisce than transverse incisions, especially in children under 1 year of age. Transverse incisions were reapproximated by individual fascial layers compared to vertical incisions, which were closed in one mass layer. In our study, the wound dehiscence rate was 1.75% in the paediatric subgroup, which falls within the published range of other studies.
Another systematic review and meta-analysis published by Tandon et al. in 2021 compared tissue adhesive to sutures for the closure of paediatric wounds and lacerations under low-tension
| [36] | Tandon S, Smale M, Pacilli M, Nataraja RM. Tissue adhesive and adhesive tape for pediatric wound closure: A systematic review and meta-analysis. J Pediatr Surg. 2021 May; 56(5): 1020-1029. https://doi.org/10.1016/j.jpedsurg.2020.07.037 |
[36]
. The analysis showed that the cosmetic outcome was not different between the devices used for wound closure, and the incidence of wound infection and dehiscence were similar between both closure groups. Individual rates after suture closure were 1.8% for wound infection and 0.6% for wound dehiscence. The authors concluded that tissue adhesives as well as sutures can be used for wound closure with equivalent risk of wound infection and wound dehiscence.
In our paediatric subgroup we found a wound infection rate of 3.51% (2/57) and a wound dehiscence rate of 1.75%. In interpreting our subgroup results for children, it is important to consider that most previous studies evaluated clean/uncomplicated wounds which are at low risk of infection. In these studies, an infection rate of 1.2% - 6.6% has been reported in children
| [37] | Bhattacharyya N, Kosloske AM. Postoperative wound infection in pediatric surgical patients: a study of 676 infants and children. J Pediatr Surg. 1990 Jan; 25(1): 125-9. https://doi.org/10.1016/s0022-3468(05)80177-0 |
| [38] | Horwitz JR, Chwals WJ, Doski JJ, Suescun EA, Cheu HW, Lally KP. Pediatric wound infections: a prospective multicenter study. Ann Surg. 1998 Apr; 227(4): 553-8. https://doi.org/10.1097/00000658-199804000-00017 |
| [39] | Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20. https://doi.org/10.1007/s003830000389 |
[37-39]
.
Furthermore, previous studies performed in paediatrics could demonstrate that the wound infection rate is associated with the duration of operation and wound contamination
| [37] | Bhattacharyya N, Kosloske AM. Postoperative wound infection in pediatric surgical patients: a study of 676 infants and children. J Pediatr Surg. 1990 Jan; 25(1): 125-9. https://doi.org/10.1016/s0022-3468(05)80177-0 |
| [39] | Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20. https://doi.org/10.1007/s003830000389 |
[37, 39]
. The authors stated that wound infections in children are related more to the factors at operation than to the overall physiologic status of the patient
| [37] | Bhattacharyya N, Kosloske AM. Postoperative wound infection in pediatric surgical patients: a study of 676 infants and children. J Pediatr Surg. 1990 Jan; 25(1): 125-9. https://doi.org/10.1016/s0022-3468(05)80177-0 |
| [39] | Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20. https://doi.org/10.1007/s003830000389 |
[37, 39]
. Battacharyya et al. analysed the wound infection rate in a paediatric population including neonates, infants and children
. Overall wound infection rate was 2.5%, with 0.7% in neonates, 4.1% in infants and 2.3% in children, respectively. No difference was found regarding gender, but the infection rate was associated with the contamination class (clean 1%, clean-contaminated 2.9%, contaminated 7.9% and dirty 6.3%) and increased with the length of hospital stay (outpatient 1.7% versus 0-48h in-hospital stay 3.0%). The authors found the highest wound infection rate after gastrointestinal surgery (3.7%) and after respiratory tract surgery (5%), compared to inguinal hernia repair (2.1%) or operations on skin or soft tissue (2.1%). In our study, both SSI occurred after hernia repair (1x inguinal and 1x umbilical hernia) in the paediatric group. Battacharyya et al. concluded that wound infection is associated with operative procedures longer than 1 hour, with urgency of the operation and with additional illness or disease of the patient. Local factors such as wound contamination, tissue perfusion, and tissue handling play a more important role in the determination of paediatric wound infection than the general condition of the patient. They also stated that infants under 1 year of age undergoing inguinal herniorrhaphy were more likely to develop a wound infection than older patients (4% vs. 0%), probably caused by bacterial contamination within the diaper
.
In our series, the wound infections occurred in children aged 9 and 12. The wound infection rate reported by Battacharyya et al. for this age group was 2.3% compared to 3.5% in our cohort, showing no severe difference
. In addition, Battacharyya et al. mentioned that the wound infection rate increases with operation duration. Surgeries performed under 1 hour showed an infection rate of 0.6%, whereas procedures over 1 hour had an infection rate of 2.9%
. The average duration of surgery was 22.28 ±8.66 minutes in the paediatrics subgroup of our study, ranging from 10.00 min. to 50.00. min.
Uludag et al. performed a prospective study to investigate the incidence of surgical site infections in paediatric patients
| [39] | Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20. https://doi.org/10.1007/s003830000389 |
[39]
. They reported an infection rate of 6.6%, which was twice as high compared to our rate (3.5%). Emergency procedures, an operation duration over 1 hour and inpatients showed a statistically higher risk for the development of wound infections. Furthermore, they mentioned that most of the wound infections occurred within the 2
nd week after the operation (82%) in their study
| [39] | Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20. https://doi.org/10.1007/s003830000389 |
[39]
. This can be confirmed by our results, because one SSI was seen after 7 days after surgery and the second one after 8 days postoperatively.
We found neither wound infection nor wound dehiscence in the adult group. Several studies mentioned higher SSI rates in adults than in children and the results of our study (0.0%) do not support that conclusion
| [37] | Bhattacharyya N, Kosloske AM. Postoperative wound infection in pediatric surgical patients: a study of 676 infants and children. J Pediatr Surg. 1990 Jan; 25(1): 125-9. https://doi.org/10.1016/s0022-3468(05)80177-0 |
| [39] | Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20. https://doi.org/10.1007/s003830000389 |
[37, 39]
. Previously mentioned infection rates in adults depending on contamination class were as follows: 1.5 – 5.5% for clean, 7.7% - 10.8% for clean-contaminated 15.2% -21.9 contaminated and up to 40% for dirty
. A large review of wound dehiscence in adult patients reported an incidence between 1-3%
| [42] | Poole GV Jr. Mechanical factors in abdominal wound closure: the prevention of fascial dehiscence. Surgery. 1985 Jun; 97(6): 631-40. |
[42]
.
The outcome of the wound appearance was assessed in the SKINDA study as an effective parameter. The review of the literature performed by Shin et al. supports the use of subcuticular closure over simple interrupted stitches or simple running suture on the trunk and extremities for improved cosmetic outcome
| [43] | Shin TM, Bordeaux JS. How suture technique affects the cosmetic outcome of cutaneous repairs. J Drugs Dermatol. 2014 Aug; 13(8): 967-9. |
[43]
. In 14 studies that included 1,473 subjects consisting of 39% females and 61% males with an average age of 45.9 years ranging from 18 months to 78 years and undergoing mainly abdominal surgery (36%) and laparoscopic /endoscopic interventions (11%) with the need of an incision mostly at the trunk/extremities (95%) indicated that subjects and observers rating scars repaired by subcuticular technique to have a better overall appearance using the Vancouver and Hollander scar score. In the SKINDA study, patients and observers used the POSAS for scar assessment. Independently of the assessor and subgroup (adults or paediatrics), an excellent aesthetic outcome was found, whereby in children mainly the intracutaneous-continuous suture technique (93%) and in adults the transcutaneous-interrupted suture technique (91%) were selected for skin closure. This indicates that the positive cosmetic result seen after the usage of a nylon-based suture material was independent of the used suture technique, in contrast to Shin et al. The excellent aesthetic scar outcome in our study was further confirmed by a high satisfaction of the study population and a beneficial wound healing assessment by the physician at any point of judgement.
Another prospective study published by Fontana et al. compared systematically the short- and long-term complications and aesthetic outcome of fascial laceration in children
| [44] | Fontana S, Schiestl CM, Landolt MA, Staubli G, von Salis S, Neuhaus K, Mohr C, Elrod J. A Prospective Controlled Study on Long-Term Outcomes of Facial Lacerations in Children. Front Pediatr. 2021 Feb 12; 8: 616151. https://doi.org/10.3389/fped.2020.616151 |
[44]
. The skin closure was done either using tissue glue or suture material (non-absorbable nylon suture or absorbable PGLA) and the POSAS was rated by 5 different plastic surgeons. The POSAS overall evaluation for the suture group showed 3.0; 95% CI [2.91-3.17] for the observer component and 3.5; 95% CI [3.22-3.84] for the patient component. We obtained the following values for the paediatric group: overall observer component 2.32±0.54 at suture removal and 2.13 ±0.33 at 1 month postoperatively, for the overall patient component 1.88±0.94 at suture removal and 2.25±0.56 at 1 month postoperatively. These findings indicate a better aesthetic outcome for children in our study compared to the study performed by Fontana et al. Furthermore, their wound dehiscence rate was much higher with 3.7% in the suture group compared to 1.75% in our series. Nevertheless, Fontana et al. concluded that both modalities of wound closure (suture and tissue glue) yielded favourable aesthetic results, and complications were rare
| [44] | Fontana S, Schiestl CM, Landolt MA, Staubli G, von Salis S, Neuhaus K, Mohr C, Elrod J. A Prospective Controlled Study on Long-Term Outcomes of Facial Lacerations in Children. Front Pediatr. 2021 Feb 12; 8: 616151. https://doi.org/10.3389/fped.2020.616151 |
[44]
.
Regarding the intra-operatively handling of the suture material, all dimensions were predominantly judged as very good to excellent during the surgeries performed in the adult group. The paediatric surgeons rated the tensile strength and the tissue drag as excellent in all surgeries and the categories (pliability, knot run down and knot security) received a good to very good assessment, whereby in 9 paediatric surgeries “knot security” obtained only a satisfied evaluation. This shows that paediatric surgeons were more critical regarding the knot security of suture materials compared to surgeons doing adult surgeries. It is known that non-absorbable suture materials tend to have higher suture memory making them springy with a tendency for the knots to unravel compared to absorbable sutures. This point and handling category seem to be more important for paediatric surgeons compared to other surgeons.
The strengths of the current SKINDA study are the multicentric design, two subgroups with equivalent patient distribution and 99% follow-up examination of the cohort until suture removal. The study is limited regarding sample size, use of a historic control group and short-term follow- up until 30 days after surgery.
5. Conclusions
The SKINDA study, a multicentric, international, prospective cohort study, could demonstrate that a nylon-based suture material is safe to use for skin closure in adults as well as in paediatrics after a variety of surgical interventions. Independently of the selected suture technique, an excellent cosmetic result was obtained in the adult and paediatric population, with a high patient satisfaction and a beneficial wound/scar assessment by the physician. The present findings confirmed that a monofilament, non-absorbable, nylon suture material is a good alternative to other devices, which are currently in use to approximate the wound edges of surgical incisions located at the trunk and limbs. Further research on this topic should be made and future studies should focus on a high quality design including clinical objectives as well as patient´s reported outcome parameter.
Abbreviations
BMI | Body Mass Index |
DCR | Data Clarification Request |
CDC | Centers for Disease Control and Prevention |
CRF | Case Report Form |
Max | Maximum |
Mean | Average |
Min | Minimum |
NCT | ClinicalTrials.gov Identifier |
POSAS | Patient and Observer Scar Assessment Scale |
SSI | Surgical Site Infection |
SD | Standard Deviation |
STROCCS | Strengthening the Reporting of Cohort Studies in Surgery |
USP | United States Pharmacopeia |
VAS | Visual Analogue Scale |
Acknowledgments
The authors would like to thank Viktor Breul who was responsible for sample size calculation and data analysis. Special thanks to Irene Fita who performed the monitoring visits in the Spanish Hospital.
Author Contributions
Petra Baumann: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Project administration, Validation, Writing – original draft
Manuel Lopez: Data curation, Investigation, Writing – review & editing
Jessica Hoelderle: Data curation, Investigation, Writing – review & editing
Jan Ludolf Kewer: Data curation, Investigation, Writing – review & editing
Funding
The study was sponsored and funded by B. Braun Surgical SA, Rubi, Barcelona, Spain. The Sponsor has also covered the costs for publication.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Kujath P, Michelsen A. Wounds - from physiology to wound dressing. Dtsch Arztebl Int. 2008 Mar; 105(13): 239-48.
https://doi.org/10.3238/arztebl.2008.0239
|
| [2] |
Rodrigues M, Kosaric N, Bonham CA, Gurtner GC. Wound Healing: A Cellular Perspective. Physiol Rev. 2019 Jan 1; 99(1): 665-706.
https://doi.org/10.1152/physrev.00067.2017
|
| [3] |
Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res. 2010 Mar; 89(3): 219-29.
https://doi.org/10.1177/0022034509359125
|
| [4] |
Singh R, Hawkins W. Sutures, ligatures and knots. Surgery (Oxford), 2020, 38(3), 123-127,
https://doi.org/10.1016/j.mpsur.2020.01.003
|
| [5] |
Edlich RF, Gubler K, Wallis AG, Clark JJ, Dahlstrom JJ, Long WB 3rd. Wound closure sutures and needles: a new perspective. J Environ Pathol Toxicol Oncol. 2010; 29(4): 339-61.
https://doi.org/10.1615/jenvironpatholtoxicoloncol.v29.i4.60
|
| [6] |
Dennis C, Sethu S, Nayak S, Mohan L, Morsi YY, Manivasagam G. Suture materials - Current and emerging trends. J Biomed Mater Res A. 2016 Jun; 104(6): 1544-59.
https://doi.org/10.1002/jbm.a.35683
|
| [7] |
Luck RP, Flood R, Eyal D, Saludades J, Hayes C, Gaughan J. Cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations. Pediatr Emerg Care. 2008 Mar; 24(3): 137-42.
https://doi.org/10.1097/PEC.0b013e3181666f87
|
| [8] |
Luck R, Tredway T, Gerard J, Eyal D, Krug L, Flood R. Comparison of cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations. Pediatr Emerg Care. 2013 Jun; 29(6): 691-5.
https://doi.org/10.1097/PEC.0b013e3182948f26
|
| [9] |
Theopold C, Potter S, Dempsey M, O'Shaughnessy M. A randomised controlled trial of absorbable versus non-absorbable sutures for skin closure after open carpal tunnel release. J Hand Surg Eur Vol. 2012 May; 37(4): 350-3.
https://doi.org/10.1177/1753193411422334
|
| [10] |
Moy RL, Waldman B, Hein DW. A review of sutures and suturing techniques. J Dermatol Surg Oncol. 1992 Sep; 18(9): 785-95.
https://doi.org/10.1111/j.1524-4725.1992.tb03036.x
|
| [11] |
Hochberg J, Meyer KM, Marion MD. Suture choice and other methods of skin closure. Surg Clin North Am. 2009 Jun; 89(3): 627-41.
https://doi.org/10.1016/j.suc.2009.03.001
|
| [12] |
Fowler JR, Perkins TA, Buttaro BA, Truant AL. Bacteria adhere less to barbed monofilament than braided sutures in a contaminated wound model. Clin Orthop Relat Res. 2013 Feb; 471(2): 665-71.
https://doi.org/10.1007/s11999-012-2593-z
|
| [13] |
Lekic N, Dodds SD. Suture Materials, Needles, and Methods of Skin Closure: What Every Hand Surgeon Should Know. J Hand Surg Am. 2022 Feb; 47(2): 160-171.e1.
https://doi.org/10.1016/j.jhsa.2021.09.019
|
| [14] |
Malhotra K, Bondje S, Sklavounos A, Mortada H, Khajuria A. Absorbable versus Nonabsorbable Sutures for Facial Skin Closure: A Systematic Review and Meta-analysis of Clinical and Aesthetic Outcomes. Arch Plast Surg. 2024 Jun 19; 51(4): 386-396.
https://doi.org/10.1055/a-2318-1287
|
| [15] |
Xu B, Xu B, Wang L, Chen C, Yilmaz TU, Zheng W, He B. Absorbable Versus Nonabsorbable Sutures for Skin Closure: A Meta-analysis of Randomized Controlled Trials. Ann Plast Surg. 2016 May; 76(5): 598-606.
https://doi.org/10.1097/SAP.0000000000000418
|
| [16] |
Al-Abdullah T, Plint AC, Fergusson D. Absorbable versus nonabsorbable sutures in the management of traumatic lacerations and surgical wounds: a meta-analysis. Pediatr Emerg Care. 2007 May; 23(5): 339-44.
https://doi.org/10.1097/01.pec.0000270167.70615.5a
|
| [17] |
Sajid MS, McFall MR, Whitehouse PA, Sains PS. Systematic review of absorbable vs non-absorbable sutures used for the closure of surgical incisions. World J Gastrointest Surg. 2014 Dec 27; 6(12): 241-7.
https://doi.org/10.4240/wjgs.v6.i12.241
|
| [18] |
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996 Feb; 17(1): 1-12.
https://doi.org/10.1016/0197-2456(95)00134-4
|
| [19] |
Agha RA, Borrelli MR, Vella-Baldacchino M, Thavayogan R, Orgill DP; STROCSS Group. The STROCSS statement: Strengthening the Reporting of Cohort Studies in Surgery. Int J Surg. 2017 Oct; 46: 198-202.
https://doi.org/10.1016/j.ijsu.2017.08.586
|
| [20] |
Draaijers LJ, Tempelman FR, Botman YA, Tuinebreijer WE, Middelkoop E, Kreis RW, van Zuijlen PP. The patient and observer scar assessment scale: a reliable and feasible tool for scar evaluation. Plast Reconstr Surg. 2004 Jun; 113(7): 1960-5; discussion 1966-7.
https://doi.org/10.1097/01.prs.0000122207.28773.56
|
| [21] |
van de Kar AL, Corion LU, Smeulders MJ, Draaijers LJ, van der Horst CM, van Zuijlen PP. Reliable and feasible evaluation of linear scars by the Patient and Observer Scar Assessment Scale. Plast Reconstr Surg. 2005 Aug; 116(2): 514-22.
https://doi.org/10.1097/01.prs.0000172982.43599.d6
|
| [22] |
Truong PT, Lee JC, Soer B, Gaul CA, Olivotto IA. Reliability and validity testing of the Patient and Observer Scar Assessment Scale in evaluating linear scars after breast cancer surgery. Plast Reconstr Surg. 2007 Feb; 119(2): 487-94.
https://doi.org/10.1097/01.prs.0000252949.77525.bc
|
| [23] |
Foster GE, Hardy EG, Hardcastle JD. Subcuticular suturing after appendicectomy. Lancet. 1977 May 28; 1(8022): 1128-9.
https://doi.org/10.1016/s0140-6736(77)92385-6
|
| [24] |
Kotaluoto S, Pauniaho SL, Helminen M, Kuokkanen H, Rantanen T. Wound healing after open appendectomies in adult patients: a prospective, randomised trial comparing two methods of wound closure. World J Surg. 2012 Oct; 36(10): 2305-10.
https://doi.org/10.1007/s00268-012-1664-3
|
| [25] |
Lundblad R, Simensen HV, Wiig JN, Niels Grüner OP. Hudlukning. [Skin closure. A prospective randomized study]. Tidsskr Nor Laegeforen. 1989 Apr 30; 109(12): 1307-9.
|
| [26] |
Pauniaho SL, Lahdes-Vasama T, Helminen MT, Iber T, Mäkelä E, Pajulo O. Non-absorbable interrupted versus absorbable continuous skin closure in pediatric appendectomies. Scand J Surg. 2010; 99(3): 142-6.
https://doi.org/10.1177/145749691009900308
|
| [27] |
Ralphs DN, Cannon SR, Bolton JP. Skin closure of inguinal herniorrhaphy wounds in short-stay patients. Br J Surg. 1982 Jun; 69(6): 341-2.
https://doi.org/10.1002/bjs.1800690617
|
| [28] |
Szabó S, István G. Inguinális sérvmútétek bórvarrata gyorsan felszívódó Polyglactin 910/370 (Vicryl-Rapide) fonallal [Skin closure in inguinal hernia repair with rapidly absorbing Polyglactin 910/370 (Vicryl-Rapide) suture material]. Magy Seb. 2002 Apr; 55(2): 77-80.
|
| [29] |
Niederstaetter IM, Schiefer JL, Fuchs PC. Surgical strategies to promote healing. Med. Sci. 2021, 9(45).
https://doi.org/10.3390/medsci9020045
|
| [30] |
Simman R. Wound closure and the reconstructive ladder in plastic surgery. J Am Col Certif Wound Spec. 2009 May 1; 1(1): 6-11.
https://doi.org/10.1016/j.jcws.2008.10.003
|
| [31] |
Vogt PM, Altintas MA, Radtke C, Meyer-Marcotty M. Grundlagen und Techniken der chirurgischen Naht [Bases and methods of suturing]. Chirurg. 2009 May; 80(5): 437-44, 446-7. German.
https://doi.org/10.1007/s00104-009-1670-7
|
| [32] |
Luo W, Tao Y, Wang Y, Ouyang Z, Huang J, Long X. Comparing running vs interrupted sutures for skin closure: A systematic review and meta-analysis. Int Wound J. 2023 Jan; 20(1): 210-220.
https://doi.org/10.1111/iwj.13863
|
| [33] |
Waldhausen JH, Davies L. Pediatric postoperative abdominal wound dehiscence: transverse versus vertical incisions. J Am Coll Surg. 2000Jun; 190(6): 688-91.
https://doi.org/10.1016/s1072-7515(00)00284-2
|
| [34] |
Singer AJ, Thode HC Jr. A review of the literature on octylcyanoacrylate tissue adhesive. Am J Surg. 2004 Feb; 187(2): 238-48.
https://doi.org/10.1016/j.amjsurg.2003.11.017
|
| [35] |
Campbell DP, Swenson O. Wound dehiscence in infants and children. J Pediatr Surg. 1972 Apr; 7(2): 123-6.
https://doi.org/10.1016/0022-3468(72)90485-x
|
| [36] |
Tandon S, Smale M, Pacilli M, Nataraja RM. Tissue adhesive and adhesive tape for pediatric wound closure: A systematic review and meta-analysis. J Pediatr Surg. 2021 May; 56(5): 1020-1029.
https://doi.org/10.1016/j.jpedsurg.2020.07.037
|
| [37] |
Bhattacharyya N, Kosloske AM. Postoperative wound infection in pediatric surgical patients: a study of 676 infants and children. J Pediatr Surg. 1990 Jan; 25(1): 125-9.
https://doi.org/10.1016/s0022-3468(05)80177-0
|
| [38] |
Horwitz JR, Chwals WJ, Doski JJ, Suescun EA, Cheu HW, Lally KP. Pediatric wound infections: a prospective multicenter study. Ann Surg. 1998 Apr; 227(4): 553-8.
https://doi.org/10.1097/00000658-199804000-00017
|
| [39] |
Uludag O, Rieu P, Niessen M, Voss A. Incidence of surgical site infections in pediatric patients: a 3-month prospective study in an academic pediatric surgical unit. Pediatr Surg Int. 2000; 16(5-6): 417-20.
https://doi.org/10.1007/s003830000389
|
| [40] |
Public Health Laboratory Service: incidence of surgical wound infections in England and Wales: A report of the Public health Laboratory Service Great Britain. Lancet 1960; 2: 659-663.
https://doi.org/10.1016/S0140-6736(60)91742-6
|
| [41] |
Cruse PJ, Ford R. The epidemiology of wound infection. A 10-year prospective study of 62,939 wounds. Surg Clin North Am. 1980 Feb; 60(1): 27-40.
https://doi.org/10.1016/s0039-6109(16)42031-1
|
| [42] |
Poole GV Jr. Mechanical factors in abdominal wound closure: the prevention of fascial dehiscence. Surgery. 1985 Jun; 97(6): 631-40.
|
| [43] |
Shin TM, Bordeaux JS. How suture technique affects the cosmetic outcome of cutaneous repairs. J Drugs Dermatol. 2014 Aug; 13(8): 967-9.
|
| [44] |
Fontana S, Schiestl CM, Landolt MA, Staubli G, von Salis S, Neuhaus K, Mohr C, Elrod J. A Prospective Controlled Study on Long-Term Outcomes of Facial Lacerations in Children. Front Pediatr. 2021 Feb 12; 8: 616151.
https://doi.org/10.3389/fped.2020.616151
|
Cite This Article
-
APA Style
Baumann, P., Lopez, M., Hoelderle, J., Kewer, J. L. (2024). Assessment of a Non-Absorbable Monofilament Suture for Skin Closure in Adults and Paediatrics – Skinda, an International, Bi-Centric, Prospective Cohort Study. Journal of Surgery, 12(6), 139-154. https://doi.org/10.11648/j.js.20241206.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Baumann, P.; Lopez, M.; Hoelderle, J.; Kewer, J. L. Assessment of a Non-Absorbable Monofilament Suture for Skin Closure in Adults and Paediatrics – Skinda, an International, Bi-Centric, Prospective Cohort Study. J. Surg. 2024, 12(6), 139-154. doi: 10.11648/j.js.20241206.13
Copy
|
Download
AMA Style
Baumann P, Lopez M, Hoelderle J, Kewer JL. Assessment of a Non-Absorbable Monofilament Suture for Skin Closure in Adults and Paediatrics – Skinda, an International, Bi-Centric, Prospective Cohort Study. J Surg. 2024;12(6):139-154. doi: 10.11648/j.js.20241206.13
Copy
|
Download
-
@article{10.11648/j.js.20241206.13,
author = {Petra Baumann and Manuel Lopez and Jessica Hoelderle and Jan Ludolf Kewer},
title = {Assessment of a Non-Absorbable Monofilament Suture for Skin Closure in Adults and Paediatrics – Skinda, an International, Bi-Centric, Prospective Cohort Study
},
journal = {Journal of Surgery},
volume = {12},
number = {6},
pages = {139-154},
doi = {10.11648/j.js.20241206.13},
url = {https://doi.org/10.11648/j.js.20241206.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20241206.13},
abstract = {Each surgical incision has to be closed after surgery. Suture materials are mostly applied which differ in their filament structure, material composition, as well as in their absorption profile, and the choice of the suture material used for skin closure is mainly based on the surgeon´s preference. We designed a prospective, international, multicentric, single-arm, observational study to assess the clinical outcome of a non-absorbable monofilament nylon-based suture for skin closure with a comparison to historic data from the literature. In total, 115 patients were enrolled with an equally distribution of adults and paediatrics receiving a nylon-based suture material to close the skin. Different safety (wound dehiscence, surgical site infections, and adverse events) and effectiveness parameters (pain, wound healing, patient satisfaction, cosmetic result, intraoperative suture handling) were selected to judge the performance of the suture material. The assessment of patient satisfaction, wound healing, and handling properties of the suture was done using a Likert scale, whereas the Patient and Observer Scar Assessment Scale (POSAS) was chosen for aesthetic scar rating. The primary endpoint was a combined rate of wound dehiscence and surgical site infection occurring until suture removal. After discharge, the patients were examined at suture removal and the paediatric population received a further routinely 1-month post-surgery follow-up. Until suture removal, 2 surgical site infections (1.75%) occurred and one wound dehiscence was seen until 30 days postoperatively, indicating significant lower rates compared to historical data. Furthermore, good handling properties of the suture material as well as a high patient satisfaction combined with an excellent wound healing and cosmetic appearance were reported. Based on our findings, it can be concluded that a monofilament nylon-based suture material is an optimal choice for skin closure in adults as well as in children, and it represents an appropriate alternative to other devices, which are currently in utilization.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessment of a Non-Absorbable Monofilament Suture for Skin Closure in Adults and Paediatrics – Skinda, an International, Bi-Centric, Prospective Cohort Study
AU - Petra Baumann
AU - Manuel Lopez
AU - Jessica Hoelderle
AU - Jan Ludolf Kewer
Y1 - 2024/12/10
PY - 2024
N1 - https://doi.org/10.11648/j.js.20241206.13
DO - 10.11648/j.js.20241206.13
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 139
EP - 154
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20241206.13
AB - Each surgical incision has to be closed after surgery. Suture materials are mostly applied which differ in their filament structure, material composition, as well as in their absorption profile, and the choice of the suture material used for skin closure is mainly based on the surgeon´s preference. We designed a prospective, international, multicentric, single-arm, observational study to assess the clinical outcome of a non-absorbable monofilament nylon-based suture for skin closure with a comparison to historic data from the literature. In total, 115 patients were enrolled with an equally distribution of adults and paediatrics receiving a nylon-based suture material to close the skin. Different safety (wound dehiscence, surgical site infections, and adverse events) and effectiveness parameters (pain, wound healing, patient satisfaction, cosmetic result, intraoperative suture handling) were selected to judge the performance of the suture material. The assessment of patient satisfaction, wound healing, and handling properties of the suture was done using a Likert scale, whereas the Patient and Observer Scar Assessment Scale (POSAS) was chosen for aesthetic scar rating. The primary endpoint was a combined rate of wound dehiscence and surgical site infection occurring until suture removal. After discharge, the patients were examined at suture removal and the paediatric population received a further routinely 1-month post-surgery follow-up. Until suture removal, 2 surgical site infections (1.75%) occurred and one wound dehiscence was seen until 30 days postoperatively, indicating significant lower rates compared to historical data. Furthermore, good handling properties of the suture material as well as a high patient satisfaction combined with an excellent wound healing and cosmetic appearance were reported. Based on our findings, it can be concluded that a monofilament nylon-based suture material is an optimal choice for skin closure in adults as well as in children, and it represents an appropriate alternative to other devices, which are currently in utilization.
VL - 12
IS - 6
ER -
Copy
|
Download